您好,欢迎访问三七文档
当前位置:首页 > 商业/管理/HR > 其它文档 > 最新反流性食管炎治疗进展-PPT文档
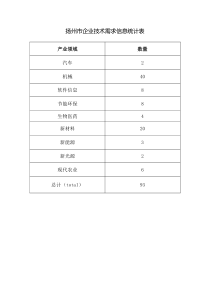
省医消化反流性食管炎RefluxEsophagitis(R.E.)定义:酸碱反流导致的食管粘膜破损Esophagealmucosalbreaks=Esophagealmucosalerosionorulceration2、Accepted-AEvidence-A省医消化胃食管反流病(GERD)Gastroesophagealrefluxdisease定义:胃或十二指肠内容物反流入食管所致的临床症状或食管粘膜组织结构改变省医消化食管炎流行病学西方国家烧心反流症状发生率10-20%北京上海调查:GER症状8.97%GERD5.77%RE1.92%中国一项研究:内镜检查5.8%有RE80%非心源性胸痛由GERD引起省医消化GERD流行病学GERD在全球范围内正迅速成为上消化道最常见疾病Hp根除导致产酸增加体重增加脂肪摄入增加体力活动减少的生活方式暂时性下食管括约肌松弛(10-15秒以上)食管裂孔疝是发生GERD的两个主要原因GuidoNJTytgat1999.12.省医消化AcidandbilerefluxinerosiveGERD0%20%40%60%80%100%01,23,4Esophagitisgrade%ofpatientsNopathologicalrefluxPathologicalacidrefluxPathologicalbilefefluxPathologicalmixedrefluxMadrid1999.3省医消化Bilerefluxinpatientswithpartialgastrectomies051015202530TotalUprightSupineTimeabsorbanceo.14(%)controlcisaprideMadrid1999.3省医消化碱性反流性食管炎•碱性环境中非结合胆酸水溶性,损伤食管粘膜PH3.5-7.0,胰蛋白酶活性维持90分钟•酸性环境中,结合胆酸水溶性↑,损伤食管粘膜•胰液中卵磷脂在磷指酶A的作用下,形成溶血卵磷脂,破坏食管粘膜。省医消化RE的内镜分型Savary-Miller分型(1978年)I级:一处或多处贲门上方非融合性的粘膜损害、红斑伴或不伴有渗出或表浅糜烂II级:融合性糜烂渗出病变,但未完全累积食管全周III级:糜烂或溃疡波及食管全周,但未引起狭窄IV级:慢性粘膜病变或溃疡、管壁纤维化、缩短、瘢痕化伴Barrett食管省医消化RE内镜分型食管炎的东京分型(1996年)O级:食管无异常发现I级:发红或白色混浊II级:糜烂、溃疡在齿状线上5cm以内未波及1/4周径III级:糜烂、溃疡在齿状线上5-10cm可见有融合者但未及全周,溃疡不及1/4周径IV级:糜烂达全周或在齿状线10cm以上,溃疡超过1/4周径注:Barrett有或无、长度,狭窄有或无、直径。省医消化RE内镜分型中国RE内镜诊断及分级(1999年8月25日烟台)分级食管粘膜内镜下表现积分O级正常(可有组织学改变)0I级点状或条状发红、糜烂无融合现象1II级有条状发红、糜烂,并有融合但非全周性2III级病变广泛、发红、糜烂融合呈全周性或有溃疡3注明:各病变部位(食管上、中、下段)和长度;狭窄部位、直径和长度;Barrett食管改变部位,有无食管裂孔疝省医消化TheLosAngelesClassificationSystemfortheendoscopicassessmentofoesophagitisGradeDefinitionAOneormoremucosalbreaksnolongerthan5mm,noneofwhichextendsbetweenthetopsofthemucosalfoldsBOneormoremucosalbreaksmorethan5mmlong,noneofwhichextendsbetweenthetopsoftwomucosalfoldsCMucosalbreaksthatextendbetweenthetopsoftwoormoremucosalfolds,butwhichinvolvelessthan75%oftheoesophagealcircumferenceDMucosalbreakswhichinvolveatleast75%oftheoesophagealcircumference省医消化食管炎洛杉矶内镜分型A、至少一处粘膜破损(Mucosalbreaks)病变长度不超过5mm,宽度不超过相邻两条粘膜皱壁B、至少一处粘膜破损病变长度超过5mm,宽度不超过相邻两条粘膜皱壁C、粘膜破损宽度超过两条以上粘膜皱壁但不及75%食管周径D、粘膜破损超过75%食管周径粘膜破损=粘膜糜烂或溃疡省医消化RE的诊断大多数具有反流症状的病人无内镜下食道炎目前内镜技术水平对充血红斑、脆性增加等微小病变的诊断不可靠cannotbedetectedreliablywithcurrentendoscopytechnologies强调反流症状在诊断中的重要性、烧心特异性90%24小时pH监测对PPI治疗效差的病人评估省医消化PLACEOFpHMONITORINGANDOTHERINVESTIGATION30Accepted-A:Twentyfourhouresophagealacidexposureisnotsufficientlysensitiveforittoserveasadiagnosticgoldstandardforrefluxdisease.Evidence-A:Normalacidexposurevaluesarerecordedinuptoaquarterofpatientswithotherwisetypicalrefluxesophagitis,andinaboutonethirdofpatientswithendoscopynegativerefluxdisease.Theclassificationofnormal/abnormalacidexposurechangesinaminorityofpatientswhentheyarestudiedasecondtime.Coregroup:thesubstantiallimitationofthediagnosticsensitivityofesophagealacidexposurevaluesisnotwidelyrecognised.From:Anevidence-basedappraisalofrefluxdiseasemanagement--TheGenvalWorkshopReport省医消化RE的治疗目的:控制症状,防治并发症,预防复发。一般治疗:抬高床头,戒烟酒,低脂低糖,避免饱食。药物治疗:PPI2次/日*8周,剂量减半维持至少6月。H2RA促动力药,3-4次/日,并维持治疗碱反流加用达喜、硫糖铝外科治疗:药物无效或有并发症可考虑。省医消化改变生活方式•Stressedtheimportanceofanearlyeveningmeal•减少脂肪摄入,尤晚餐•避免咖啡、巧克力干扰LES功能•减少体重•抬高床头:严重夜间反流11thAPCGE,2000,Hongkong省医消化GERD是常见病美国成人10%,每天烧心40%,曾经烧心20%,可能出现溃疡、狭窄、Barrett’s食管2001.DDW.Atlanta省医消化GERD是慢性复发性疾病停止治疗,迅速发生,需长程治疗“低剂量维持疗法”,80%病人6月后复发,建立标准剂量维持治疗2001.DDW.Atlanta省医消化教育病人改变生活方式多数GERD是慢性终身性疾病改变生活方式是有效治疗的基础backbone25%病人改变生活方式症状控制高枕、避免饱餐脂餐、餐后直立位至少2小时戒烟,选用OTC控制症状2001.DDW.Atlanta省医消化H2拮抗剂和动力(AmpleEvidence)充分证据可控制50%GERD症状轻中度食管炎有效单用-联用-加大剂量-联用2001.DDW.Atlanta省医消化PPI治疗GERD最有效胃、食管PH监测对治疗效差,病人有益了解夜间酸分泌高水平和伴发的反流合理剂量,长期治疗,100%GERD有效11年长期随访,证明PPI安全性2001.DDW.Atlanta省医消化抗反流手术作用明确的手术指征仍有争论3年随访发现,内科药物,外科手术同样有效Losec治疗反流性食管炎有效、安全真正的内科治疗无效者少见充足剂量定时服药45-50岁者考虑手术,费用/效益比佳2001.DDW.Atlanta省医消化GERD小结GERD是慢性复发性疾病,需终身治疗内科药物,外科手术都是有效的治疗选择2001.DDW.Atlanta省医消化Upperabdominal/lowerrestrosternalsymptomsSymptomevaluationSymptomsconsistentwithrefluxDeterminesymptomseveritySymptomstroublesome=RefluxdiseaseNoalarmsymptomManageempiricallyDistinguishsevereoesophagitisPromptendoscopyAlarmsymptomOtherSymptomManageaccordingtopatternDyspepsiaManageasdyspepsiaReassure/non-drugmeasuresPromptendoscopyNoalarmsymptomAlarmsymptomSymptomsmildandinfrequentMajorstrategies,evaluationsanddecisionsformanagement省医消化NotendoscopedorendoscopednegativeorLosAngelesAorBoesophagitisH2RAorCisaprideHighdosePPI2-4weeksSymptompersistentHighdosePPI1-2weeksSymptomspersistentSymptomspersistentSymptomscontrolledEndoscopyifnotyetdoneReassesssymptoms,pHmonitoringDominantpathway省医消化LosAngelesgradeCorDoesophagitisFulldosePPI8weeksDoubledosePPI8weeksSymptomspersistentSymptomspersistentSymptomscontrolledSymptomscontrolledReassesssymptomsendoscopypHmonitoringContinuefulldosePPIAntirefluxsurgeryContinuedoubledosePPIAntirefluxsurgeryDoubleorhigherdosePPIOesophagitisHealedEndoscopyOesophagitisEndoscopyHealedPatientcategoryInitialtherapyLongtermmanagement省医消化SuccessfulinitialdrugtherapySymptomrecurrenceTrialofwithdrawalofdrugtherapyNosymptomrecurrenceNotpreviouslyendoscopedEndoscopyLosAngelesCorDoesophagitisRestartsuccessfulinitialdrugtherapyEndoscopynegative:LosAngelesAorBoesophagitisSevereoesophagitisprotocolContinueoffdrugth
 三七文档所有资源均是用户自行上传分享,仅供网友学习交流,未经上传用户书面授权,请勿作他用。
三七文档所有资源均是用户自行上传分享,仅供网友学习交流,未经上传用户书面授权,请勿作他用。
 扫描二维码
扫描二维码



 korey_chiu
korey_chiu
本文标题:最新反流性食管炎治疗进展-PPT文档
链接地址:https://www.777doc.com/doc-1394300 .html